Free Florida Dh 3212 Form
Understanding Florida Dh 3212
-
What is the Florida DH 3212 form?
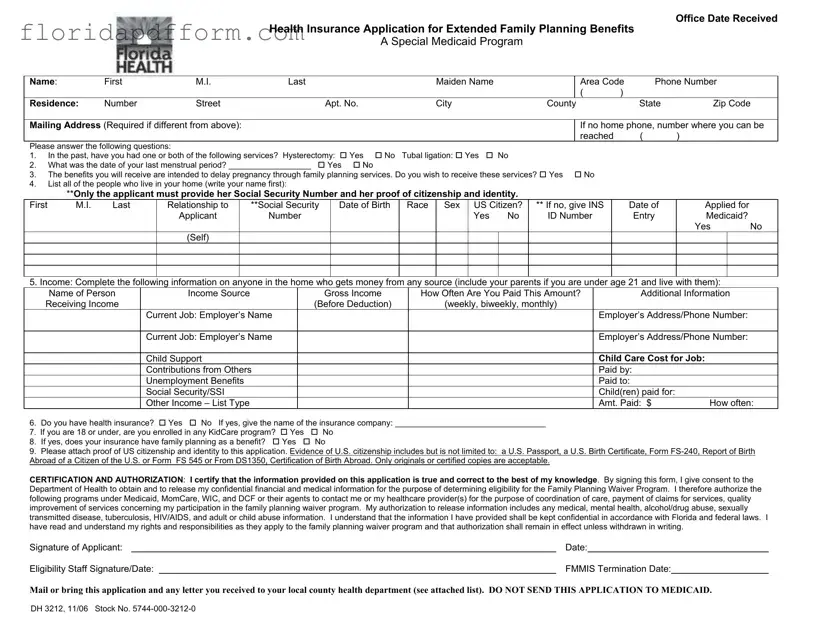
The Florida DH 3212 form is an application for Health Insurance for Extended Family Planning Benefits. It is specifically designed for individuals seeking to access the Medicaid Family Planning Waiver program. This program provides essential family planning services to eligible individuals who have lost their full Medicaid coverage.
-
Who is eligible to apply for the Family Planning Waiver program?
To qualify for the Family Planning Waiver program, you must meet certain criteria:
- You must have lost your full Medicaid coverage.
- You should not have undergone a hysterectomy or tubal ligation.
- You must not be currently pregnant.
- You should express a desire for family planning services.
- Your income must be less than or equal to 185% of the current federal poverty level.
-
What information do I need to provide on the form?
The form requires various details, including:
- Your name, address, and contact information.
- Your reproductive history regarding hysterectomy or tubal ligation.
- A list of individuals living in your household, including their relationship to you.
- Income details for everyone in your home.
- Health insurance information, if applicable.
- Proof of U.S. citizenship and identity.
-
How do I submit the application?
You should mail or bring the completed DH 3212 form to your local county health department. It is important not to send the application directly to Medicaid. Ensure that you include any required documentation, such as proof of citizenship and income.
-
What happens after I submit my application?
Once you submit your application, the health department will review it to determine your eligibility for the Family Planning Waiver program. You may be contacted for additional information, and you will receive a notification by mail regarding your eligibility status.
-
What should I do if I need assistance with the application?
If you require help completing the application or have questions, consider reaching out to your local health department. They can provide guidance and support to ensure that your application is filled out correctly and submitted on time.
Common mistakes
-
Incomplete Personal Information: Many individuals neglect to provide complete personal information, such as their full name, address, and phone number. This omission can lead to delays in processing the application.
-
Failure to Answer All Questions: Some applicants skip questions, particularly those related to reproductive history and family planning desires. Each question is essential for determining eligibility, and incomplete responses can hinder the process.
-
Missing Required Documentation: Applicants often forget to attach proof of U.S. citizenship and identity. Without this documentation, the application cannot be processed, resulting in potential denial of benefits.
-
Incorrect Income Reporting: Many people inaccurately report their income or fail to include all household members who contribute financially. This error can affect eligibility and the level of benefits received.
-
Not Signing the Application: Some applicants overlook the importance of signing and dating the application. A missing signature renders the application invalid, causing unnecessary delays in receiving assistance.
How to Use Florida Dh 3212
Completing the Florida DH 3212 form is a crucial step in applying for extended family planning benefits through Medicaid. This application gathers essential information to determine eligibility for the program. To ensure a smooth process, follow these steps carefully, as each section plays a vital role in your application.
- Begin by entering the office date received at the top of the form.
- Fill in your name (first, middle initial, last, and maiden name) in the designated fields.
- Provide your phone number with area code.
- Complete your residence address, including street number, apartment number (if applicable), city, county, state, and zip code.
- If your mailing address differs from your residence, fill in the mailing address section.
- If you don’t have a home phone, provide an alternative contact number.
- Answer the questions in the reproductive history section (questions 1-3) by marking 'Yes' or 'No' as applicable.
- For question 4, list all individuals living in your home, starting with your name. Include their relationship to you, Social Security Number, date of birth, race, sex, and whether they are a U.S. citizen. If not, provide the INS number and date of entry.
- In question 5, document the income for each person in your household who receives money. Include their name, income source, gross income, and how often they are paid.
- Answer question 6 regarding health insurance. If applicable, provide the name of your insurance company.
- For questions 7 and 8, indicate your enrollment in any KidCare program and whether your insurance covers family planning benefits.
- Attach proof of U.S. citizenship and identity to your application, ensuring you use originals or certified copies.
- Read the Certification and Authorization section carefully, then sign and date the form.
- Finally, mail or bring the completed application to your local county health department. Do not send it to Medicaid.
File Specs
| Fact Name | Details |
|---|---|
| Form Purpose | The DH 3212 form is used to apply for the Health Insurance Application for Extended Family Planning Benefits in Florida. |
| Eligibility Criteria | To qualify, applicants must not have had a hysterectomy or tubal ligation, must not be pregnant, and must desire family planning services. |
| Income Requirement | Applicants must have an income that is less than or equal to 185% of the current federal poverty level. |
| Required Information | Only the applicant needs to provide a Social Security Number and proof of citizenship and identity. |
| Submission Instructions | Applicants must mail or bring the completed form to their local county health department. It should not be sent to Medicaid. |
| Confidentiality Assurance | Information provided on the form will be kept confidential in accordance with Florida and federal laws. |
| Governing Laws | This form operates under Florida Statutes, particularly those related to Medicaid and family planning services. |
Additional PDF Forms
Fl Medical Board - Health conditions that might prevent normal school activity participation should be noted.
Is a Sellers Disclosure Required in Florida - Any known restrictions regarding leasing the property must be shared.
Florida Realtors Lease Agreement Pdf - The contract establishes a time frame for acceptance, specifying a deadline for signatures.