Free First Report Of Injury Florida Form
Understanding First Report Of Injury Florida
-
What is the First Report of Injury Florida form?
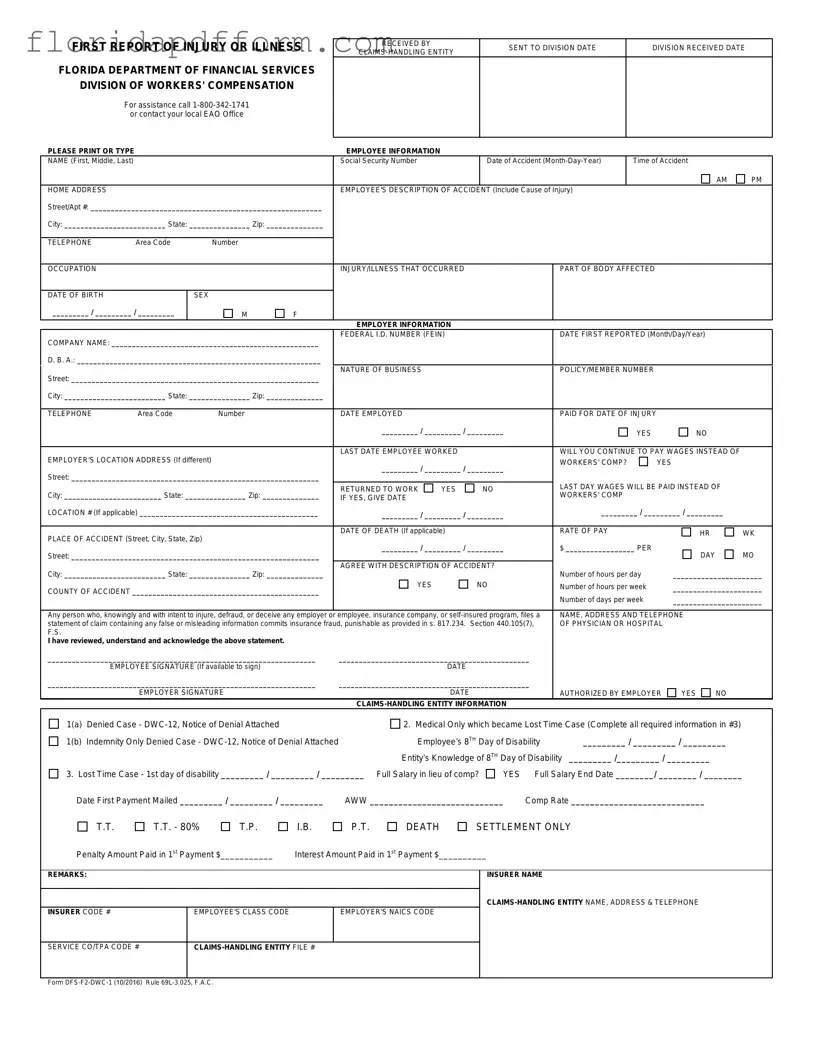
The First Report of Injury form is a crucial document used in Florida to report workplace injuries or illnesses. It is required by the Florida Department of Financial Services and is part of the workers' compensation process. This form collects essential information about the injured employee, the employer, and the nature of the injury. Completing this form accurately is vital for ensuring that the injured worker receives the benefits they are entitled to.
-
Who is responsible for filing the First Report of Injury form?
Typically, the employer is responsible for filing the First Report of Injury form. However, the injured employee can also submit the form if the employer fails to do so. It’s important for employers to act quickly, as timely reporting can affect the benefits the employee may receive. If you are an employee, make sure to communicate with your employer about the accident and encourage them to file the report promptly.
-
What information is needed to complete the form?
Completing the form requires several pieces of information. You'll need to provide details about the employee, including their name, Social Security number, and date of birth. Additionally, information about the accident is essential, such as the date and time of the incident, a description of how it happened, and the nature of the injury. Employer details, including the company name and address, are also necessary. Gathering this information beforehand can help streamline the filing process.
-
What happens after the form is submitted?
Once the First Report of Injury form is submitted, it is sent to the Division of Workers' Compensation. They will review the report and determine the next steps regarding the claim. The employer and employee will receive updates about the claim status and any required actions. It's important for both parties to keep communication open and follow up as needed, ensuring that all necessary documentation is provided in a timely manner.
Common mistakes
-
Incomplete Employee Information: Failing to fill out all required fields, such as the employee's name, social security number, or date of accident, can lead to delays in processing the claim. Make sure every section is completed thoroughly.
-
Vague Description of the Accident: Providing a general or unclear description of how the injury occurred can create confusion. Be specific about the cause of the injury and include all relevant details.
-
Incorrect Employer Information: Entering the wrong company name or federal ID number can result in the claim being misdirected. Double-check that all employer details are accurate.
-
Missing Dates: Omitting critical dates, such as the date of injury or last date worked, can stall the claims process. Ensure that all date fields are filled out correctly.
-
Neglecting to Sign: Not signing the form can invalidate the report. If the employee is unavailable to sign, make sure the employer or authorized representative does so.
-
Failure to Report All Injuries: Sometimes, individuals only report the most obvious injury. It’s important to include all injuries sustained during the incident, even if they seem minor, as they may affect the claim.
How to Use First Report Of Injury Florida
Once you have gathered all the necessary information, filling out the First Report of Injury form is straightforward. This form is essential for documenting workplace injuries and begins the process for workers' compensation claims. Follow these steps carefully to ensure accuracy and completeness.
- Obtain the form: You can find the First Report of Injury form on the Florida Department of Financial Services website or request a copy from your employer.
- Fill in the received by section: Indicate who received the form and the date it was received.
- Complete employee information: Write the employee's full name, Social Security number, and date of the accident. Include the time of the accident (AM or PM) and the home address.
- Describe the accident: Provide a detailed description of how the injury occurred, including the cause of the injury.
- Provide contact information: Enter the employee's telephone number and occupation.
- Detail the injury: Specify the injury or illness that occurred and which part of the body was affected. Include the employee's date of birth and sex.
- Fill in employer information: Enter the company name, federal ID number, and the date the injury was first reported. Also, include the "Doing Business As" (D.B.A.) name, if applicable, and the nature of the business.
- Provide the employer's address: If the employer's location is different, fill in that address as well.
- Document employment details: Indicate the date the employee was hired, whether they were paid for the date of injury, and the last date they worked.
- Wages information: State whether the employer will continue to pay wages instead of workers' compensation and provide the last day wages will be paid.
- Accident location: Fill in the place of the accident, including the street, city, state, and zip code.
- Complete additional sections: If applicable, provide information on the employee's death, agree or disagree with the description of the accident, and fill in the number of hours worked per day, week, and days per week.
- Sign the form: The employee should sign and date the form if available. The employer must also sign and date it, indicating if they are authorized to do so.
- Submit the form: Once completed, submit the form to the appropriate claims-handling entity as instructed.
After submitting the form, it will be processed by the claims-handling entity. They will review the information and determine the next steps regarding the workers' compensation claim. Keep a copy of the completed form for your records, as it may be needed for future reference.
File Specs
| Fact Name | Details |
|---|---|
| Purpose | The First Report of Injury form is used to report workplace injuries or illnesses to the Florida Department of Financial Services. |
| Governing Law | This form is governed by Florida Statutes, specifically Chapter 440, which outlines workers' compensation laws. |
| Submission Deadline | The form must be submitted within 7 days of the employer's knowledge of the injury or illness. |
| Required Information | Key information includes employee details, accident description, employer information, and the nature of the injury. |
| Fraud Warning | Filing false information on this form can lead to charges of insurance fraud, as stated in Section 440.105(7), Florida Statutes. |
| Contact Information | For assistance, individuals can call 1-800-342-1741 or reach out to their local Employee Assistance Office. |
Additional PDF Forms
Parenting Plan Agreement Template - A parenting plan may need to be created if you and the other parent cannot reach an agreement.
Tabla De Child Support Florida En Español - This form facilitates a structured approach to calculating child support amounts.
Florida F-1120 Instructions - Consultations with tax professionals may be beneficial to ensure correct filing of the F-1120.